二. 若以手術後 牙肉有沒有完全縫合蓋回 來區分.....
早期 Branemark 植體 建議植牙後牙肉應完全縫合回去 讓埋入的植體在完全不受外力干擾下 達成骨整合... 待六個月後 做第二次手術 把植體接出口腔來 再等數週 牙肉癒合後 方可印模做假牙 ... 這種需兩次手術的方式 稱之為 "二階式植牙術式"(Two-stage impant placement procedure)
之後ITI植體廠商 推出的植體 其smooth collar 長度2.8mm 種入齒槽骨時 直接穿過牙肉 露出於口腔 挑戰 Branemark 的植牙原則 植牙手術後 直接接出於口腔 待三個月後 直接印模做假牙 不需要二次手術.... 這種只需一次手術的方式 稱之為 "一階式植牙術式"(One-stage implant placement procedure)
ITI 植體 可見光滑區 2.8mm ....

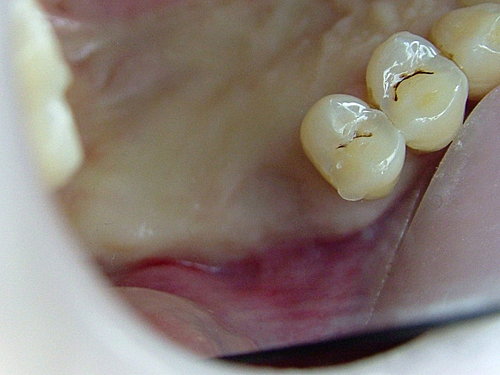
植牙前 .. 後牙缺了兩棵大牙....
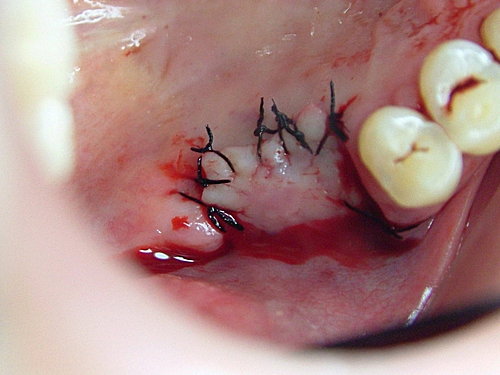
植牙手術後 將牙肉缝回....
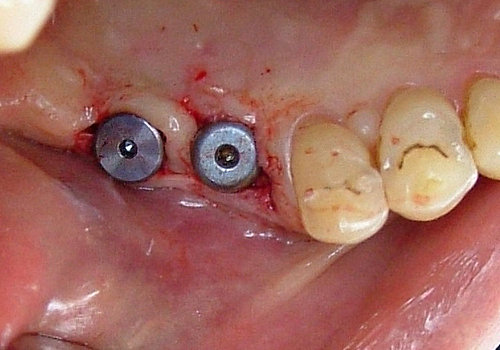
等三個月骨整合後 做二次手術 接上牙齦癒合樁柱(healing abutment) 讓植體接出於口腔 再等數週 牙齦癒合成形後 就可取模 裝上假牙了!! 這就是 "Two -tage approach"....
"One-stage approach" 如下.... 兩側後牙皆缺牙 ~

手術植牙後 直接接上 healing abutment 再將牙肉縫合 等三個月後 就可直接印模 ....

如果有興趣的話 還可以參考以下文章 ~
Two Stage vs. One Stage – Is There Really A Controversy?
By David A. Garber, DMD, Henry Salama, DMD, and Maurice A. Salama, DMD
Introduction
The long held injunction setting the two-stage implant approach as the standard
surgical modality is derived from the original Branemark protocol developed in the
1960’s and 1970’s. This protocol was designed as a solution for the totally edentulous
patient to support a removable or hybrid type replacement prosthesis. The initial working
premise for the two stage approach was that the successful development of
osseointegration at the bone implant site during the healing phase.
Animal and clinical research conducted over the last ten years, however, have
convincingly proven that a one stage protocol can deliver an equal level of predictability
to the achievement of osseointegration. Indeed, the present state of knowledge has
rendered as moot, any discussions comparing the two or one stage approaches solely
based on their ability to achieve oseointegration. Instead, relevant comparisons of the
two approaches now focus on their ability to promote clearly defined clinical endpoints
such as patient management, esthetics and peri-implant tissue health. Towards that end,
therapeutic decision making must emphasize the matching of surgical protocols with the
appropriate implant design based on the specific parameters inherent at the receptor site
(Table 1).
We have identified specific clinical parameters that directly affect the choices
made. These parameters are categorized as follows:
I. Implant placement is the mature site.
Esthetic anterior vs. posterior implant placement
A) In posterior or edentulous implant placement a one stage surgical protocol and
a one stage implant design, i.e. with a polished collar of 1.5-3mm offers distinct
advantages. These advantages include easier and more efficient patient management
because there is only one surgical intervention. In addition, optimal management of the
peri-implant biological width is enhanced by moving the implant/restorative microgap
above the osseous crest.
B) In anterior esthetic applications, however, the soft tissue demands create
significant challenges that alter decision making. Even proponents of one stage implant
systems have proposed altering their surgical protocols in the anterior region to include a
two stage protocol of deeper than usual fixture placement which negates the advantages
listed earlier for the placement in the posterior region.
It is, therefore, clear that soft tissue and esthetic demands will effect the choice of a one
or two stage implant protocol as well as a one or two stage implant design.
II. Immediate extraction protocol – two or one stage
Esthetic concerns determine that a tooth destined for extraction should be
evaluated prior to tooth removal to comprehensively evaluate the potential implant
receptor site. If it is within the esthetic zone, the necessity of the underlying osseous
topography being present to support the soft tissue profiles of the restorative recipient site
is essential. Esthetic soft tissue predictability necessitates the presence of interdental
osseous peaks of bone within 5mm of the contact point of the potential final restoration.
If deficient, soft tissue profiles and the underlying osseous housing may be augmented
prior to extraction utilizing orthodontic manipulation of the tooth in an incisal direction.
Following an atraumatic extraction, (without raising a flap/incisionless) the residual
socket is now evaluated to ascertain if it is intact or if there is compromise in the labial or
lingual osseous plate – which may take the form of either a dehiscence or a fenestration.
The advent of wide platform fixtures dramatically altered the immediate implant
technique. The matching diameter of the implant body and that of the socket eliminated
the need for a membrane over the top of the socket to allow for G.B.R. in the gap
between the fixture and the socket in the coronal portion. If these wide bodied fixtures
were directed somewhat lingual to the original socket, they could often be placed in the
native bone with primary stability while obliterating the access to the socket thereby not
requiring a membrane and G.B.R. (This eliminated the need for a definitive two stage
procedure and a healing abutment could then be used in the conventional one stage
approach.) If the site is intact, the sequential drilling ostectomies are preformed and the
site once again evaluated for perforation of the bony housing. If none exists, the implant
may be placed in a one stage nonsubmerged approach. (Fig. A and B – 135, 139)
Perforation of the socket during the sequential drilling ostectomies for cylindrical
traditional implants can often be eliminated by using a fixture design that decreases in
diameter towards the apical region to accommodate the labial concavity in the premaxilla
– no osseous compromise facilitates a one stage approach and expedites the process.
However, if either following extraction or the drilling ostectomies the integrity of
osseous housing has been compromised a flap may now need to be raised. In our
opinion, if the osseous compromise is a dehiscence the two stage approach becomes
necessary. In these cases, the bone is invariably lost on the labial surface and following
implant placement, primary stability is evident but threads may be exposed thru the
osseous housing. In these cases membrane guided bone regeneration may be utilized in
conjunction with some form of grafting material to maintain space below the membrane.
A two stage implant design is generally easier to use in these cases as the reduced profile
facilitates complete flap closure.
The tissue must now be advanced coronally


請先 登入 以發表留言。